From Fee-for-Service to Value-Based Care: A Provider’s Guide
Confused by the evolution from Fee-for-Service to Capitation? Equus Growth breaks down the risks and trade-offs of Value-Based Care and helps providers navigate the changing economics of healthcare delivery.




I was speaking with a friend who advises companies in sales and marketing. He had never worked in healthcare but recently signed a client focused on value-based care (VBC). He asked if I could help him understand what that means. As we discussed the topic, I realized that many people—inside and outside the industry—don’t fully understand the evolution of our healthcare system nor where it may be headed. That’s one reason we created Equus Growth: to help providers manage through the ever-evolving nature of providing care.
For decades, most insurance plans have reimbursed providers through fee-for-service (FFS). In FFS, the more visits, tests, or procedures a provider delivers, the more revenue is generated. A patient typically starts with primary care or urgent care, then is referred for imaging and often a specialist. The insurer pays each provider for each service, with the patient contributing a co-payment.
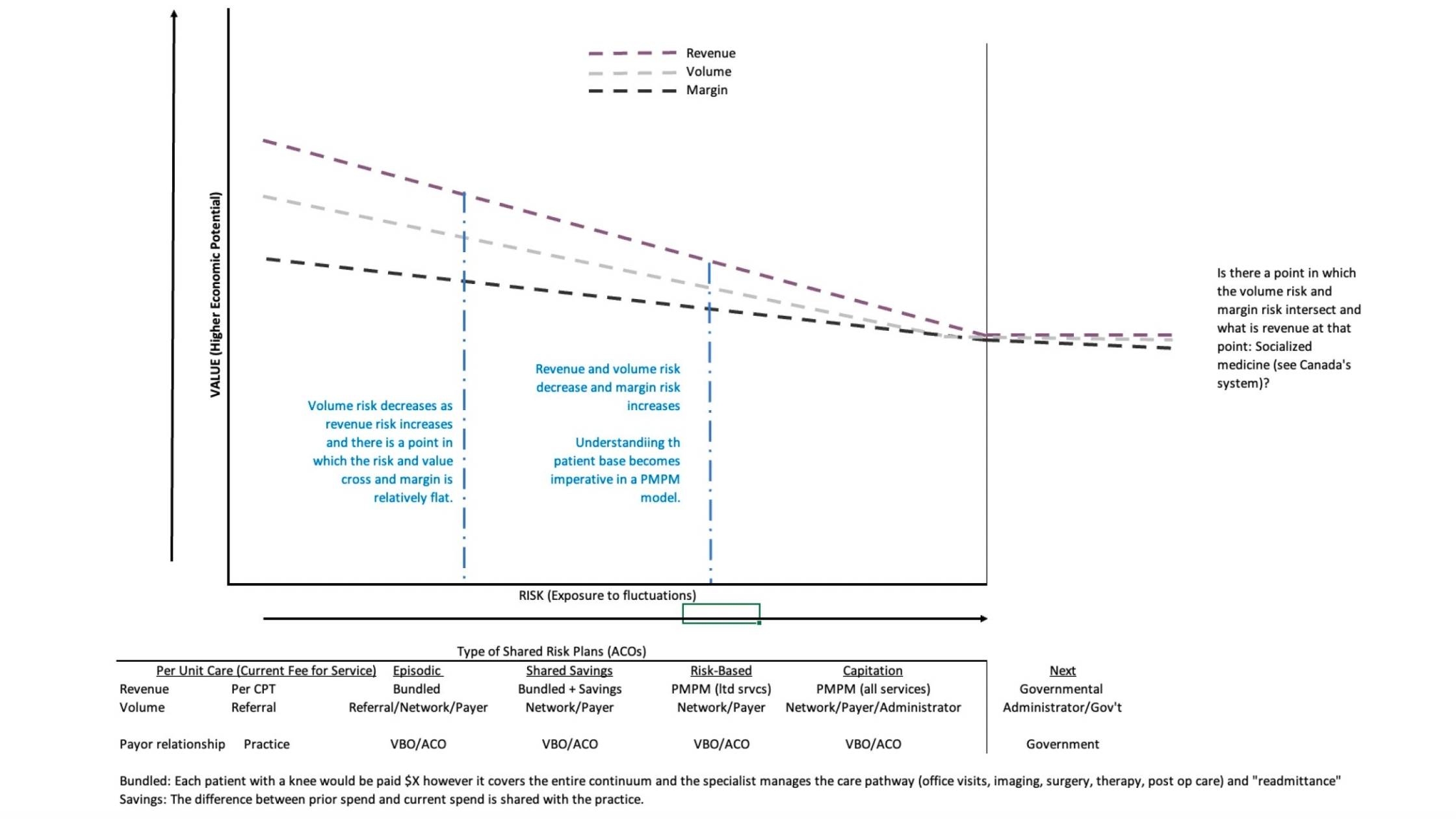
Over the last decade, the system has increasingly shifted toward models that focus on the continuum of care rather than each individual episode. One major step in that direction is episodic care / bundled payments, where a provider agrees to a predetermined payment for an entire course of care—imaging, surgery, office visits, therapy, and follow-up. Patients may still be referred to other providers, but insurers steer them toward in-network participants in the episodic model. The payment is bundled, and it becomes the provider’s responsibility to manage the care pathway effectively. This often creates lower revenue per episode and more margin pressure. The provider trades the margin risk for more patient volume.
Many of these arrangements are administered through Insurance Companies, Value-Based Care Organizations (VBOs) or Accountable Care Organizations (ACOs) (collectively, “Administrators”), which contract with the government and insurance companies to administer the reimbursement programs. As these networks scale, they may also participate in shared savings—for example, if historical spend for a service line was $4M and the most recent year is $3M, the Administrator and network participants share a portion of the $1M savings. This creates positive incentives and a reduction in overutilization often seen in FFS. However, it shifts significant risk away from insurers and toward Administrators and providers.
As VBC continues to evolve, contracts increasingly move to per-member per-month (PMPM) arrangements. Early “risk-based” versions may apply to specific conditions or service lines, and over time can progress to capitation, where providers assume responsibility for essentially the entire continuum of care for a fixed PMPM amount. While capitation is not new, it represents a meaningful risk transfer and can create incentives to delay care or make decisions based on margin, triaging what is urgent and risk rather than patient need.
Healthcare tends to be cyclical, and past consolidation cycles offer lessons. The difference now is that the government (Medicare/Medicaid) is the one consolidating through Advantage and administered plans. Continued pressure could reduce the number of Administrators/Insurance companies, increasing centralized control of healthcare through control of payment—and therefore the delivery—of healthcare resulting in a nationalized healthcare. There is no perfect system; every structure has trade-offs. Providers, however, must manage increasing risk with decreasing reward—and that is where Equus Growth can help. Please reach out to us to discuss your plan and strategy in the ever-evolving healthcare industry.