
ACOs, Value-Based Care, and Integrated Networks
This white paper explains how ACOs, value-based care, and integrated care networks are reshaping healthcare payment in the U.S. It outlines what these models mean for rehabilitation providers and shows how PTs, OTs, PTAs, OTAs, and SLPs can demonstrate their value through outcomes, cost avoidance, data tracking, and stronger partnerships with primary care and ACOs.




ACOs, Value-Based Care, and Integrated Networks
Executive Summary
The way healthcare gets paid for in the United States is undergoing the biggest restructuring in a generation. Fee-for-service is shrinking. Value-based care is rising. Accountable Care Organizations, alternative payment models, and integrated systems like Kaiser Permanente are now the language of how money flows from payers to providers.
For physical therapy, occupational therapy, and speech-language pathology practices, this shift is more than a policy update. It is a chance to be paid for the outcomes the profession has always delivered. Functional improvement. Avoided surgeries. Lower fall risk. Shorter stays in skilled nursing facilities. These are the outcomes that move the financial needle inside a value-based contract, and rehab clinicians measure them every day.
This paper traces how the United States arrived at value-based care, defines the major payment models, walks through real-world examples, and closes with a practical playbook for any rehab provider who wants a seat at the table.
Why This Conversation Matters Now
Healthcare is changing. The way we pay for care, the way we deliver it, the way we measure whether it worked. Every clinician who touches a patient will feel this shift, including PTs, OTs, and SLPs. It changes how we think about the full patient journey, where we add the most value inside that journey, and how we partner with the rest of the care team to give the people we serve one connected experience.
If you work in rehab today, the temptation is to treat payment model conversations like background noise. They are not. They are reshaping the financial and clinical ground we stand on. The clinicians who understand the new language will be ready to pivot. The ones who don’t will be playing catch-up.
This white paper covers the basics about the new payment paradigms. We will review the history of medical payment, define the different types of models in use today, walk through how they work in the real world, and end with what all of this means for rehab providers who want a seat at the table.
A Short History of How We Got Here
Medicine has always evolved on two tracks at once. The science, and the economics. In the early colonial days, before formal medical education existed, doctors and midwives took payment in goods through bartering, not money. By the mid-1700s, several colonies adopted ‘fee schedules’ to address rising competition, climbing living costs, and a credit system that let patients walk away from their medical bills. By the late 1700s, governments began licensing doctors, and the trade moved from a goods economy to a fee-for-service (FFS) industry.
Private health insurance in its modern form took shape in the late 1920s and 1930s. In 1929, Baylor University Hospital in Dallas launched the first prepaid hospital plan, which became the template for what would later be called Blue Cross. Blue Cross plans organized nationally in the 1930s as nonprofit hospital service organizations to help members cover rising hospital and physician costs.
In 1965, the Johnson administration established Medicare as a federal program to protect older adults from medical bankruptcy as their care costs climbed with age and the absence of employer-sponsored coverage. In those early years, physicians billed patients directly at a ‘reasonable rate’ and patients submitted for reimbursement. The system gave physicians and hospitals control over what they charged Medicare, which sent the program blowing through its early spending projections.
Fast forward to the 21st century. The FFS model had built-in incentives for providers to deliver as many services to as many patients as possible. Costs outpaced inflation year after year, and the system needed to be rethought. In 2006, Michael Porter and Elizabeth Olmsted Teisberg coined the modern framing of ‘Value-Based Care’ in their book Redefining Health Care, making the case that care should be measured by value to the patient. In 2015, CMS started directing the system away from traditional FFS toward a VBC model that rewards quality over quantity.
The 2010 Patient Protection and Affordable Care Act (ACA) established formal pay-for-performance incentives for alternative payment model (APM) design within the Medicare Shared Savings Program (MSSP). The result was the physician-driven Accountable Care Organization (ACO), which initially carried only upside risk-sharing.
Five years later, in 2015, CMS partnered with the MITRE Corporation to convene the Health Care Payment Learning and Action Network (HCP-LAN). The LAN brought payers, providers, employers, patients, states, and federal agencies together around one shared goal: shift the US healthcare system toward payment models that reward value, not volume.
The result was the APM Framework, first published in January 2016 and refreshed in 2017 to absorb major new developments, including passage of the Medicare Access and CHIP (Children’s Health Insurance Program) Reauthorization Act (MACRA) and the launch of more than 100 alternative payment models by the Center for Medicare and Medicaid Innovation (CMMI). The Framework gave the entire healthcare ecosystem a common language, a classification system, and a directional roadmap.
Four principles behind the APM Framework
The APM Framework rests on four ideas worth knowing as a clinician working inside one of these models:
- Patients have to be empowered and clinicians have to feel the right incentives, or healthcare will not transform.
- Success depends on whether the system can actually support and deliver the change.
- Any payment model that ignores quality is not an APM, full stop.
- The field has to move faster into Categories 3 and 4 (more on those next) to bring costs under control. The incentives to make that move have to be big enough to pull providers along with them.
The Basics: ACOs and Value-Based Care
What makes up an ACO?
An ACO is a network of doctors, hospitals, and other providers who voluntarily coordinate care for a defined patient population. The goal is simple. Deliver better care, more efficiently, for a known group of people. ACOs operate primarily through CMS’s Medicare Shared Savings Program (MSSP) under Pay-for-Performance (P4P) incentives inside an alternative payment model. The MSSP is a physician-driven ACO that initially carried only upside risk sharing. Commercial variations developed afterward and operate under a different framework.
The ACO model could not have come together without one critical piece of infrastructure: the federally funded expansion of Electronic Health Records (EHR) into every corner of the system. EHRs let ACOs aggregate the big data that drives performance and risk calculations. Recent CMS guidelines on data exchange address the long-standing interoperability gap that blocked medical data sharing.
The nonprofit Health Level Seven International (HL7), established in 1987, is a standards development organization that sets interface standards globally. HL7 develops frameworks and standards used worldwide for health IT applications to retrieve, exchange, share, and integrate electronic health information, though adoption is voluntary. HL7 developed the Fast Healthcare Interoperability Resources (FHIR) standard to widen interoperability across systems and let third-party devices access and share health records. In the US, the Office of the National Coordinator for Health Information Technology (ONC) is the cornerstone of the 21st Century Cures Act, which enforces adoption. The future state of these standards will eventually make it possible for the frontline clinician to have access to data from various sources, including wearable health data, labs, and past medical histories from other providers.
How is Value-Based Care defined?
Value-Based Care (VBC) is a payment system that ties provider income to patient health outcomes instead of visit volume. Providers earn more when they improve health, manage chronic conditions through early intervention, and prevent the downstream costs that pile up when problems escalate. Value gets calculated by dividing the quality of health outcomes by the total cost of care.
In 2015, MACRA codified VBC reform inside CMS and defined ‘value’ from the perspective of the stakeholder. The framework is the quintuple aim:
- Better patient experience
- Improved health outcomes
- Lower cost of care delivery
- Clinician wellbeing
- Advancing health equity
At its core, VBC is a care model that centers the patient and uses an evidence-based, whole-person approach. It also recognizes the patient as a ‘consumer’ of services with a financial stake in the process. Building the patient’s healthcare self-efficacy gives them a stronger voice in how and when care is rendered.
The Four Categories of VBC Models
The HCP-LAN APM Framework groups every payment arrangement into one of four categories. Category 1 is traditional fee-for-service with no link to quality. Category 4 is full population-based payment, where the provider organization carries the entire risk for a defined population. Most of the action right now is happening in Categories 3 and 4.
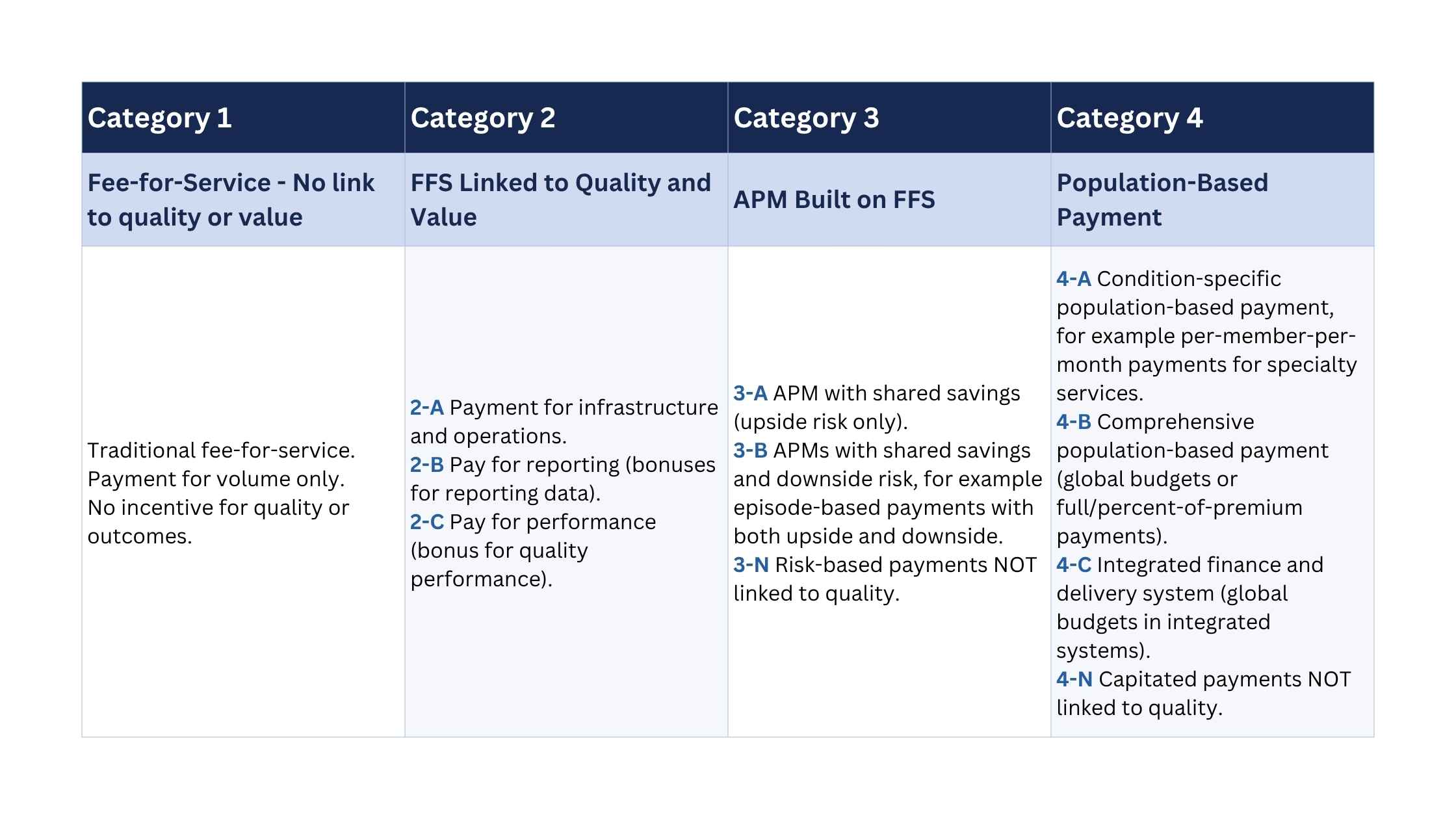
As a clinician, the question to ask about any contract on your desk is simple. Which category is this? The deeper into Categories 3 and 4 your organization sits, the more the outcomes you produce as a PT, OT, or SLP move the financial needle.
Why This Matters for Rehab
The rise of VBC and ACOs should feel like welcome news for physical, occupational, and speech therapy practices. Here is why.
FFS reimbursement, built on Relative Value Units (RVUs) and Conversion Factors (CF), keeps shrinking. CMS is stuck in a zero-sum game while Congress wrestles with how to fund care for older adults and people with disabilities. The pool of dollars is limited, whether you bill Medicare, Medicaid, or a commercial payer. Those dollars have to stretch across an entire population so that everyone has the basic foundation to live a productive, purposeful life.
The annual fight over Evaluation and Management (E/M) codes, and the constant tug of dollars between specialty care and primary care, consistently leaves rehab clinicians out in the cold. At a higher level, VBC models allocate resources to a group of providers on a risk-adjusted scale that gets distributed across the participants. That arrangement means PTs, OTs, and SLPs need to be participants in the VBC model and negotiate their value directly with the organizing entity. Knowing what problem you can solve is critical to success for every participating provider. VBC is trying to solve a complex, multifaceted problem, and two pieces deserve special attention for rehab clinicians.
The First Problem: A Fragmented Patient Journey
Start with the patient journey for people with chronic conditions and musculoskeletal (MSK) complaints. We know MSK eats one of the largest slices of healthcare spending in this country.
Musculoskeletal conditions collectively rank at the top of US health spending, alongside cardiovascular disease and diabetes. The most recent JAMA analysis of 2010 to 2019 spending put joint pain and osteoporosis at $108.6 billion. A separate analysis reported 2016 spending on low back and neck pain at $134.5 billion, osteoarthritis at $80.0 billion, and falls at $87.4 billion. Zoom out further and the picture gets harder to ignore. The CDC put the total economic cost of all US injuries in 2019 at $4.2 trillion, including $327 billion in medical care and $69 billion in work loss. These numbers tell us where the pressure is. They are the ceiling we are pressing against. To bring those costs down, we need to understand the full journey a patient takes, from the first twinge of pain to whatever comes next inside the healthcare system.
Look closely at the MSK care journey and you see fragmentation. The patient bounces between providers. The PCP, then a specialist, then imaging, then back to the PCP, then maybe a referral to a PT. Along the way, the patient juggles multiple entry points, complex scheduling, mounting co-pays, and lost time at work.
The Second Problem: Confusion About “Primary Care”
Traditionally, the PCP is the gatekeeper to everything downstream. The system has never fully supported smooth handoffs and follow-up between providers. So patients fall through the cracks. They forgo follow-up care. The condition progresses. Eventually they show up at Urgent Care or the Emergency Department. Both are expensive. Both are heavy on imaging, injections, and specialist visits. This is where rehab specialists, primarily PT, can deliver value. As an MSK primary care provider, the PT can be the gatekeeper in many instances.
The Evidence for PT-Led Primary Care
The APTA’s 2025 House of Delegates formally recognized primary care physical therapy as a specialty and residency practice. Research shows first-contact PT reduces imaging and medication use. Direct access delivers neutral to lower per-episode costs, no serious adverse events, and less burden on PCPs.
Now picture what that looks like in practice. A PT embedded in a PCP office inside an ACO, triaging MSK and chronic pain complaints at the door. One decision point. Immediate access. The PT determines who needs a single evaluation, follow-up skilled care, PTA-guided exercise, or same-day escalation to the physician. The PT works at the top of the license. The patient saves time and money. Downstream costs drop before they start.
That is the model. ACOs and VBC arrangements provide the infrastructure to make it real.

ACOs, VBC, and the Alphabet Soup of Alternative Payment Models
We have defined the VBC and APM models and categorized them. This section walks through how they operate and provides a couple of real-world examples.
How an ACO Operates
An ACO is a voluntary coalition of physicians, hospitals, and providers coordinating care for a defined Medicare population. No single entity owns it. Providers keep billing fee-for-service, but CMS watches total spend across the attributed population and compares it against a risk-adjusted benchmark at year-end. Hit the benchmark, meet the quality thresholds, keep the savings. Miss it under a two-sided risk track, and the ACO owes money back.
Quality is not a footnote here. MSSP rolls Part A and Part B into one total cost of care number, and CMS-HCC (Hierarchical Condition Category) risk scores adjust for patient complexity. Many ACO participants also contract with Medicare Advantage (MA) plans, where the incentives align around the same quality metrics, even though the financial flows stay separate.
The commercial VBC world is a different story. Every payer runs its own rules, its own reporting cadence, and its own risk stratification approach, and the complexity compounds by region. High member leakage makes longitudinal data capture difficult. Specialty bundles are emerging for joint replacement, select cardiology procedures, and maternity care, but standardization is not coming without policy pressure.
None of that complexity is a reason to wait. VBC arrangements are the future, and rehab specialists need to step into this space with confidence.
Real-World Example: MSSP at Ochsner Health
Ochsner Health System runs one of the larger MSSP ACOs in the Gulf South. Their ACO includes multiple hospitals, dozens of employed physician practices, ambulatory surgery centers, and post-acute partners. Picture a patient with knee osteoarthritis attributed to an Ochsner PCP.
The patient schedules a visit. The PCP identifies functional decline and joint pain. The care coordination team flags the patient as a candidate for conservative management before any surgical pathway. An orthopedic specialist sees the patient and, guided by ACO-aligned protocols, refers to physical therapy instead of scheduling surgery right away. The PT provider, whether employed or contracted within the ACO network, delivers a six to eight week course targeting strength, gait patterns, and pain management. Every one of those claims bills separately to Medicare FFS. At year-end, if Ochsner’s ACO population spends less than CMS’s benchmark, driven in part by avoided surgeries, shorter inpatient stays, and reduced SNF utilization, the ACO earns a shared savings check from CMS. The ACO then distributes it to participating providers per its internal agreement.
Real-World Example: Commercial Payer, BCBS Massachusetts AQC
Blue Cross Blue Shield of Massachusetts runs an Alternative Quality Contract (AQC). The AQC is a global payment model that combines a fixed per-patient payment, adjusted annually for health status and inflation, with substantial performance incentive payments tied to nationally accepted measures of quality, effectiveness, and patient experience.
That is the key structural difference from MSSP. MSSP pays fee-for-service and reconciles at year-end. The AQC gives provider organizations an annual global budget upfront so they can meet all the healthcare needs of their attributed patients. The provider group then manages total spending against that budget. They keep what they save. They absorb what they overspend.
Who participates and how it works
Members designate a primary care physician before each enrollment year. An enrollee sits inside the AQC if their PCP belongs to an organization that has joined the contract. BCBS of Massachusetts gives participating organizations technical support, including ongoing quality and spending data, to help them manage their global budgets and improve quality.
The longitudinal results are compelling. A landmark Harvard Medical School study published in the New England Journal of Medicine in 2019 found the AQC slowed the rate of medical spending growth by up to 12 percent while improving patient care over eight years. Average annual claims for patients with AQC physicians ran $461 lower than for similar patients without AQC physicians. Quality improved across several measures, including those for managing chronic conditions like diabetes and high blood pressure.
The Model That Came Before ACOs: Kaiser and Integrated Care
The Kaiser brand is recognized nationally. Kaiser Permanente was the original experiment in value-based care, a fully integrated prepaid group practice founded in 1945, more than six decades before the ACO concept existed. The current ACO is a contractual and financial structure layered onto an existing delivery system. Integrated care, like Kaiser, is the delivery system, the insurer, and the employer of clinicians, all under one brand. Current ACOs are trying to imitate this structure contractually.
The Three-Entity Structure That Makes Kaiser Unique
Kaiser Permanente (KP) is actually three interlocking organizations operating under one brand:
- Kaiser Foundation Health Plan. The insurance entity. It collects premiums, takes actuarial risk, and contracts with the other components. This is the payer.
- Kaiser Foundation Hospitals. The hospital and facility entity. It owns and operates the physical infrastructure.
- The Permanente Medical Groups. Regionally organized physician partnerships. In California there are two: The Permanente Medical Group in Northern California and Southern California Permanente Medical Group in the south. The Permanente Medical Groups are physician-owned and physician-led, and they operate exclusively inside the Kaiser ecosystem.
KP already achieves a much higher degree of integration and coordination than the MSSP ACO described earlier. In the ACO model, doctors and hospitals from different organizations work together to treat patients across the care continuum. Kaiser employs or exclusively contracts with its own clinicians. An outside rehab provider cannot share in Kaiser’s financial upside the way they can in an MSSP ACO.
Integrated care is not without its faults. The process of getting care may feel smoother, and smoother access does not always translate to better patient outcomes. Critics of the model report patients sometimes have less access, fewer choices, and certain restrictions on care. The lesson for any PCP-led care team is to put communication, collaboration, and clear protocols at the top of the priority list. Without those, team tensions develop and both quality and outcomes suffer.
Where Rehab Fits in the Financial Picture
Rehabilitation providers, especially PTs and OTs, are among the highest-impact participants in an ACO, even though their Part B billing volume is modest. Here is the math. A PT or OT can prevent SNF admissions, deflect surgical escalation, reduce readmissions, and lower fall-related ED visits. All of those reductions hit the Part A cost categories that drive ACO total cost calculations.
A PT practice billing $3,000 in Part B claims per patient can help avoid $15,000 to $30,000 in Part A costs. That value flows into the shared savings pool for the ACO entity. It does not automatically flow back to the rehab provider. Capturing it takes a contract. An ACO participant agreement with explicit gainsharing provisions, a bundled payment sub-contracting arrangement, or a commercial ACO performance program. Those contracts depend on outcome data infrastructure, episode cost transparency, and compliance with Stark Law and Anti-Kickback safe harbors. Providers who walk into these conversations with documented surgical deflection rates, functional outcome scores, and SNF avoidance data negotiate from demonstrated contribution rather than from assumption.

Pulling It All Together
ACOs, AQCs, MSSP, MA. The alphabet soup is real. Underneath the labels, the three models we walked through ask the same question. How do we pay for health, not for visits?
The answer keeps pointing back to rehab. We are the ones who see the patient over weeks, not minutes. We are the ones who know if someone can climb the stairs again, get back to work, get back on the floor with the grandkids. The outcomes that matter most to patients and to payers (function, independence, and avoided complications) are the outcomes we measure every day.
The VBC landscape is still evolving. After a decade of slow progression, the train is leaving the station at a much faster pace, and it is time to jump on before it is too late. Whether you sit inside an integrated system like Kaiser, contract with a regional MSSP ACO like Ochsner, or take referrals from a practice working under a global budget like the BCBS AQC, your value will be told by the data you collect and the relationships you build.
How a Rehab Provider Can Step In
A practical playbook for any PT, OT, PTA, OTA, or SLP reading this:
✅ Know your value. Collect and track patient-reported outcomes for every patient across the care continuum. Functional measures like TUG, Berg, the 6-minute walk test, gait parameters, pain interference, and return-to-work speak the language ACOs care about. Capture patient satisfaction alongside the clinical data.
✅ Document known downstream interventions a patient avoided. For example, imaging, injections, or surgeries the patient reports forgoing. These are your contributions to total cost of care, and they belong on a dashboard you can share with a payer or ACO partner.
✅ Use digital tools to lighten the data-capture load. Remote therapeutic monitoring (RTM) gives you longer time frames of patient activity, post-discharge tracking, and a cleaner communication line with the patient. A clean digital workflow is also a better experience for the clinician and the patient.
✅ Build a strong referral network. Have a conversation with your top referring physician about how a PT or OT in the office could triage MSK complaints and make their day easier. Meet with local orthopedic surgeons. Understand how you can help them hit benchmarks and share in gainsharing arrangements.
✅ Know who runs the ACO in your market. CMS publishes annual ACO performance data, fully public and searchable. It tells you which ACOs operate in your market, their legal names, their participant counts, and their performance history.
The CMS MSSP public listing lives here: https://data.cms.gov/medicare-shared-savings-program/accountable-care-organization-participants/data
Enter the name of a nearby hospital system. If they participate, the page lists their ACO ID number, name, and contact information for the ACO executive. That executive is your first entry point. Reach out to discuss partnerships and co-management opportunities.
✅ Learn the language of risk. HCC scores, total cost of care, two-sided risk tracks, gainsharing. The clinicians who can speak this language with administrators get invited to the table.
✅ Before you sign on the dotted line, check three things. The ACO’s financial health. Your data access. Your individual financial incentives. Targeting a collaboration with an ACO, or co-managing a bundled payment, is a much more probable path to success in the future of health than fighting for higher FFS reimbursements.
✅ Partner with primary care. PT-led primary care for MSK is a real model, supported by evidence and now by APTA policy. Look for the PCP who wants to send their MSK volume to someone they trust.
The healthcare system we trained inside is fading. The one replacing it will reward clinicians who can prove their value. Rehab has always delivered that value at the bedside, in the clinic, and in patients’ homes. The job now is to count it, document it, and translate it into the financial structures payers already use.
We have the evidence. We have the access. We have the outcomes that matter. Now is the time to claim our seat at the table.
Sources
Abuhl B, Ehrmantraut D, Wolden M. First-Contact Physical Therapy Compared to Usual Primary Care for Musculoskeletal Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phys Ther. 2025 Aug;105(8):pzaf080.
American Medical Association. What is Value-Based Care: https://www.ama-assn.org/practice-management/payment-delivery-models/what-value-based-care
Centers for Medicare and Medicaid Services. Medicare Shared Savings Program: https://www.cms.gov/medicare/payment/fee-for-service-providers/shared-savings-program-ssp-acos
Dieleman JL, Beauchamp M, Crosby SW, et al. Tracking US Health Care Spending by Health Condition and County. JAMA. 2025;333(12):1051–1061.
Dieleman JL, Cao J, Chapin A, et al. US Health Care Spending by Payer and Health Condition, 1996–2016. JAMA. 2020;323(9):863–884.
Fischer M, Bui E, Besombes L, François M. Systematic review of direct access physiotherapy for musculoskeletal conditions in primary care: consequences for general practitioner workload, resource use, and organisation of care. BMC Prim Care. 2026 Jan;27(1):75.
Gosfield AG. Beyond Face Time: The Evolution of Medicare Physician Payment. Gosfield & Associates: https://www.gosfield.com/images/PDF/BeyondFaceTime.010516.pdf
Hall MA, Schneider CE. Learning from the legal history of billing for medical fees. J Gen Intern Med. 2008 Aug;23(8):1257–60.
Harrill WC, Melon DE. A field guide to U.S. healthcare reform: The evolution to value-based healthcare. Laryngoscope Investig Otolaryngol. 2021;6:590–599.
Kaiser Permanente: https://healthy.kaiserpermanente.org/front-door
National Center for Biotechnology Information. Integrated care models: https://www.ncbi.nlm.nih.gov/books/NBK607995/
O’Bright K, Cavanaugh AM, Cassel A, et al. Primary Care Physical Therapy: 2025 Consensus Definition. Phys Ther. 2026 Apr 9:pzag035.
Performance Health. The Evolution of Health Care Costs and Reimbursement: https://www.performancehealthus.com/blog/the-evolution-of-health-care-costs-and-reimbursement
Peterson C, Miller GF, Barnett SBL, Florence C. Economic Cost of Injury, United States, 2019. MMWR Morb Mortal Wkly Rep. 2021 Dec;70(48):1655–1659.
Porter ME, Teisberg EO. How Physicians Can Change the Future of Health Care. JAMA. 2007;297(10):1103–1111.
Porter ME, Teisberg EO. Redefining Health Care: Creating Value-Based Competition on Results. Harvard Business Press; 2006.
Relay Network. Understanding HEDIS Measures: https://www.relaynetwork.com/blog/understanding-hedis-measures/
Song Z, Ji Y, Safran DG, Chernew ME. Health Care Spending, Utilization, and Quality 8 Years into Global Payment. N Engl J Med. 2019 Jul;381(3):252–263.
Yesterday’s America. Cost of Care: How Americans Have Paid for Healthcare Throughout History (2023): https://yesterdaysamerica.com/cost-of-care-how-americans-have-paid-for-healthcare-throughout-history/

